Rapid expansion of Medical Aid in Dying and forced closure of a Vancouver-area hospice have raised alarm among palliative care providers. But Peter Stockland finds vital positive signs, too.
At the beginning of April, the Supreme Court of Canada finally closed the outside door on the Delta Hospice Society’s ownership of a private 10-bed palliative care centre in suburban Vancouver.
At one level, the SCOC’s refusal to grant the Society leave to appeal lower court rulings in a bitter, year-long legal battle for control of the centre was fittingly paradoxical. The high Court had, after all, opened the door to Delta’s demise with its 2015 Carter decision that forced legalization of medical aid in dying across Canada.
MAiD, a portmanteau for the previously separate acts of euthanasia and assisted suicide, was at the centre of the political and legal fight over the Irene Thomas Centre. The Society’s board was adamant that its 30-year-old constitution did not permit MAiD on the premises. It did not object to patients who wanted an administered death being transferred to the local hospital about 100 metres away.
The compromise offer was denounced, by a local citizen’s collective aligned with the MAiD lobby group Dying with Dignity, as an affront to patients’ rights and, well, dignity. It then sought to wrest control of the Society by selling memberships door to door and otherwise in a bid to “take back Delta hospice.”
Enter the lawyers. All the way up to, or rather just shy of, the Supreme Court of Canada.
Even if the high Court had agreed to hear the case, however, its eventual decision would have been moot in any practical way. Doubling down on its legal losses, the hospice Society was also aced at the political, and most importantly, the bureaucratic level.
In late 2020, the regional Fraser Health Authority ordered eviction of the DHS board and served notice it was expropriating the Irene Thomas building as well as a neighbouring care support centre. It went so far as to enter the facility in February and advise patients at the end of their lives that they would be moved to other care centres. Concern for their rights and, well, dignity, was apparently no longer an agenda item.
In mid-March, the palliative care centre was emptied out. The last two patients were moved to other facilities. Re-opening, slated for early April, became open-ended pending resolution of issues around unionized nursing staff who were laid off because of the closure.
For board President Angelina Ireland, the Supreme Court of Canada’s refusal to permit and appeal was simultaneously no great surprise yet deeply disappointing. For much of the struggle over control, Ireland was the public face of the Delta Hospice Society side. Her trademark outspoken style was met with an onslaught of personal derision on social media and by local politicos. In hindsight, too, she recognizes that the fight was always a two-front war – both aimed at ousting the DHS board.
“We faced an air battle and a ground battle,” she says in an uncharacteristically disconsolate tone. “The air battle was from the government. The ground battle was the euthanasia activists who tried to move into the Society and force us to accept MAiD. They were working in tandem. They were going to get us one way or the other.”
Ireland says the legacy of the court cases serves as a cautionary tale to private organizations in any sphere across Canada, which is why DHS was hopeful the Supreme Court of Canada would rule private organizations cannot simply be transformed from their original mission by rent-a-crowds that purchase $10 memberships and swamp the incumbent board.
More specifically, she is convinced the closure of the small, local Irene Thomas hospice is emblematic of a national movement to have MAiD understood as integral to palliative care and, ultimately, a replacement for it. She points to the March 17 passage of federal legislation radically expanding MAiD as evidence of rapid deterioration in palliative care’s prospects for long term survivability.
“A year ago, we were hopeful that palliative care had a chance to survive in its authentic, original form. Given Bill C-7 and the actions of the B.C. government around it, there is real concern that we are not going to be able to protect palliative care,” Ireland warns.
“This 50-year model, which we know to be very clearly about helping people to live with dignity until their natural end, is ending by the sheer force of a political movement that is introducing (MAiD) into that medical model. Anyone who stands in the way of that will be dealt with very harshly,” she adds.
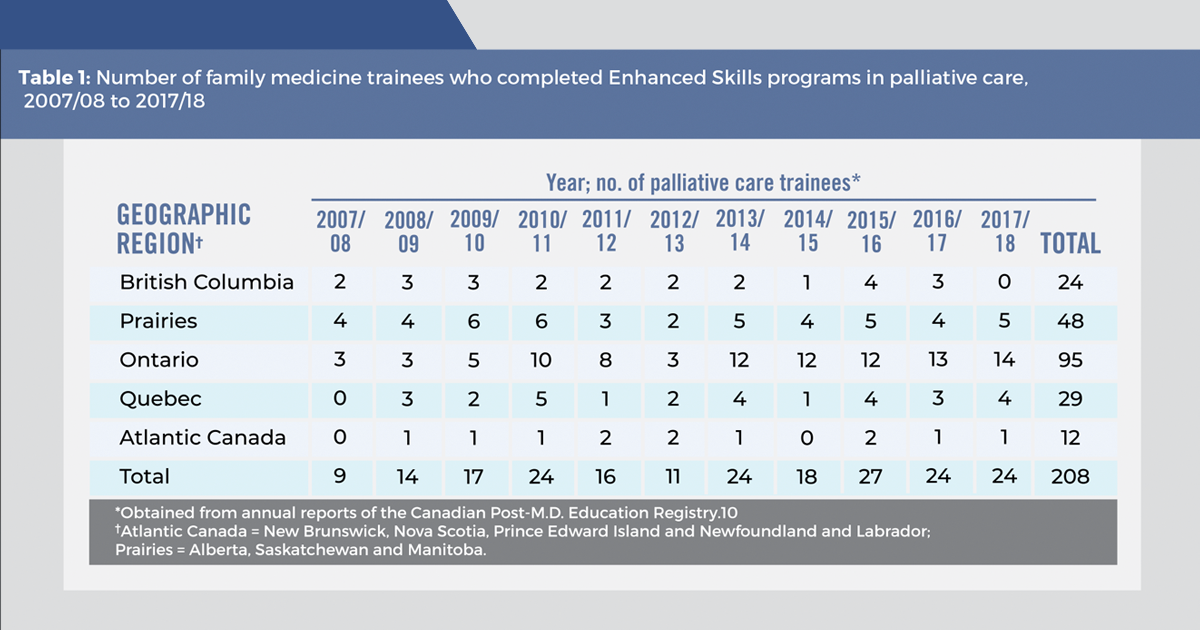
A study released in 2020, while it’s a long way from affirming Ireland’s worst fears, does give pause to consider the import of what she’s saying. The research found key training in palliative care for undergraduate and even postgraduate students is notable by its absence at medical schools across Canada.
“Without dedicated clinical exposure to palliative care, many physicians will enter practice without vital palliative care competencies,” say the six authors of the findings published in CMAJ Open, a journal of the Canadian Medical Association. “To meet current and projected palliative care needs of Canadians, most physicians should receive clinical training in palliative care, and clinical rotations are an essential component of this.”
The data shows, in fact, that just under a third of undergraduate medical students completed palliative care clinical rotations at 14 of Canada’s 17 medical schools. Three schools were dropped from the study because they were unable to provide complete data on their optional programs. Only two of the schools participating in the study make palliative care clinical rotations mandatory. Two do not offer them at all. The remainder make palliative care training optional.
At the postgraduate level, where doctors undertake intense further training in medical specialities or subspecialities, the numbers were better at almost 60 per cent for those in family medicine and about 65 per cent in geriatric medicine and psychiatry. But in neurology, internal medicine, and anesthesiology, the numbers lagged at 30 per cent or lower. The study notes that Canada’s low rates of palliative care training rotations are mirrored internationally in the U.K., the U.S., Switzerland, and Thailand.
“However, this does not justify the status quo,” it says. “In 2018 in Canada, cancer, heart and pulmonary diseases, cerebrovascular disease, diabetes mellitus, Alzheimer disease, and chronic liver disease were among the leading causes of death. All are usually preceded by prolonged and chronic illnesses….
“Physicians who have no clinical experience with palliative care may lack the necessary skills and training to care for the majority of Canadians who will die from incurable chronic illnesses,” the report’s authors add.
Dr. Anne Boyle, an associate professor of family medicine at Hamilton’s McMaster University, was one of the six authors. She says its genesis previous research showing only about 26 per cent of Canadian doctors were comfortable discussing advanced care plans and felt they needed better resources to have sound conversations around palliative care and end of life.
Boyle debunks the misconception that such concerns are relevant to only a few specialities such as geriatrics or psychiatry. She cites internal medicine as one field whose very nature recommends it for palliative care training.
“Internists deal with end-stage chronic disease as a big, significant part of their practice. It's exceedingly common for them. You would hope that they would be close to 100 per cent in having palliative care training as part of their education. But that’s not necessarily the case,” Boyle says.
Indeed, the actual figure is about 70 per cent lower. Boyle takes care, as does the study, to identify the deficiency without pointing blaming fingers. Part of the shortfall, she explains is simply a matter of finding more hours in the already jam-crammed learning schedules of medical students at both the undergraduate and postgraduate levels. Part of it is the phenomenon of the vicious cycle: the lack of palliative care training begets a lack of trainers for those who need and want to be trained.
For such practical reasons, the study stopped short of calling for mandatory palliative care clinical rotations for all Canada’s emerging medics. Still, Boyle says it’s cause for concern that only two medical schools in the country do make it mandatory – and two don’t offer it at all.
“Certainly, as an educator, that concerns me. People need to be at the bedside with an understanding of how to provide this care. We know it is important, and that it makes good economic sense. It reduces costs for delivering care, it frees up scarce resources, and it improves quality of life and quality of care for patients with serious illness – and for their families.”
When it comes to discussing MAiD potentially overwhelming palliative care, Boyle stresses the focus must remain on the clear distinction between the two. What matters is support and care for those at the end of life, she says, and on ensuring that Canadian doctors have the training skills and knowledge to carry through on those two things.
“If we don’t teach them that (as undergraduates), then I feel we’re failing our learners because we’re not giving them the tools to do the job. Then they get to post-grad and they’re like ‘well, I don’t feel comfortable with this.’
“What do we do with things we don’t feel comfortable with? We avoid them. It becomes much easier to order another test than to sit down with someone and say ‘What really matters to you? What are you willing to go through in order to have time?’ We’re not skilled at asking those questions, so they don’t get asked.”
For Dr. José Pereira, a professor and director of the palliative care division at McMaster, a key question that doesn’t get asked is how to replicate – across the country’s 17 medical schools – the successes that a few Canadian universities are having with palliative care training.
“Some programs are doing really well. Those schools should be celebrated. The question should be: What are they doing so that other schools can be doing the same?” Pereira says.
His voice carries a quarter century’s exasperation at trying to build up palliative care, including proper training, only to see last year’s small bright progress become this year’s political backslide. In the late 1990s, he was an enthusiastic participant in federal and intergovernmental planning to make palliative care a crown jewel in the Canadian medical system. Fast forward to last month as he watched the House of Commons and Senate pass Bill C-7 which will extend MAiD even to mentally ill Canadians – something unthinkable only five years ago.
There have been successes such as co-founding Pallium Canada, a country-wide organization that advances primary-level palliative care education nationally and setting up the first palliative care unit in Calgary in 2001 followed by the first formal regional palliative care program in Ontario in 2009. Then there are the moments like being stymied in getting $5,000 in funding to pay for a particular palliative care educational model. Or having a MAiD medical team invited to give a university lecture on palliative care, and Pereira being asked only to provide them a few Internet resources to explain what it is.
Over it all? For Pereira, it’s the dark wings of MAiD casting palliative care into shadow and blinding too many Canadians to the critical difference between them.
“I’ve reached a point where I’m just so demoralized,” he says. “Back in 2004, we thought that in 16 years, palliative care education would be fully integrated. Well, that’s not been the case. When my kids were growing up, I worked after hours and weekends to push for palliative care. Now, in this part of my career, at the age of 57, it’s being co-opted by (MAiD). I absolutely think that’s coming down the pipeline, and our (medical) regulatory bodies are going to be (pushing) it.”
Like Angelina Ireland, Pereira sees the current circumstance as a response to an extremely well-organized political movement driving harder and faster than most could have imagined. He notes that the study published in CMJA Open on the shortfall in palliative clinical rotations comes when training in the administration of MAiD is virtually mandatory at all Canadian medical schools. He’s also heard reliably that at least some schools are weeding out would-be doctors by pinpointing applicants who resist administering medical death.
Exasperated as he might be, at times demoralized by the sense of time running out, Pereira still firmly believes the time is right to push back on the medical schools that educate doctors, and especially on the regulatory colleges that accredit them, to finally make them raise the bar on palliative care training.
“They’re the ones that have the power to make sure the different schools integrate palliative care into education. I would ask them specifically: Why have you dropped the ball on this?”
Dr. Leonie Herx, divisional chair for palliative medicine at Queen’s University and one of palliative care’s leading Canadian advocates, says an equally compelling question is how to help Canadians inside and outside the medical establishment understand what it is.
What it’s not, she underscores, is stretching life beyond its natural elastic limits in a feckless refusal to admit the reality of death. On the contrary, it’s an extensive – though not stubbornly technologically extended – process of coming to terms with what the end of life means within the specificities of the one who will leave and those who will remain.
“The work we do in palliative care is around making sense of one’s life, one’s legacy, the story telling of how I will be remembered after I’m gone,” Herx says. “There’s a lot of rich work and healing of relationships – even if you don’t necessarily have a reunion, you can reunite with a past trauma or with a family member.
“You may in your own self be able to come to a sense of peace or healing around something that happened to you. A lot of that happens when someone’s facing their own death and is making sense of that: coming to terms with dying.”
She contrasts that process with current medical models of repeated resuscitation to help patients live by technologies rather than what they would choose given the chance to engage “those valuable conversations” about what they truly want.
“If we focus on that, people will make different decisions and we wouldn’t be in the place we’re in today where people just see you live and live and live and then you have a lethal injection and a controlled death,” Herx says.
From that perspective, she says, there should be mandatory training in palliative care at every Canadian medical school because it should be seen as a fundamental component of being a doctor. It doesn’t mean every student needs to become a specialist. It would mean core competencies in basic skills for end-of-life care.
“Every doctor needs to be comfortable with having difficult conversations, navigating complex family dynamics, decision-making around treatment options. Those should be foundational skills for any physician.
“When you’re learning about cardiology and how the heart works, you also learn about what end-stage heart disease looks like and how we manage someone’s symptoms that come about because of end-stage heart failure. You also need to learn the skills to be able to support a grieving family – grief and bereavement is a core skill in palliative care. There’s no patient or family that wouldn’t benefit from (doctors having) palliative care training,” Herx says.
The core belief behind her words is not just taken to heart but lived out daily by Dr. Krista Lawlor and her team at Montreal’s St. Raphael Palliative Care Home and Day Centre, which sits on the northeast slope of Mount Royal in the city’s Outremont borough. Despite its name, St. Raphael’s is not a faith-based institution. Yet in its origins and its ambience, the 12-bed centre embodies unmistakable continuity with the legacy of Catholic medical care dating back to Jeanne Mance and her nursing order in the 17th century, and including the Religious Hospitallers of Saint Joseph who constructed the Hotel-Dieu in the mid-19th century.
In fact, St. Raphael’s is a former parish church redeveloped on land made available by the Catholic Archdiocese of Montreal. The addition of a gorgeous, light-filled atrium entrance leads to what was not long ago the church’s basement. What used to be the bell tower calling the faithful to prayer is now, with a pixie-like bit of humour, a quiet room for use by staff, residents or their families.
Dr. Lawlor herself completed her residency in family medicine at St. Mary’s Hospital before spending four years with the Cree Board of Health and Social Services in northern Quebec’s James Bay region. Her faculty profile page for McGill University, where she is an assistant professor of family medicine and associate in the department of oncology, spells out that it was her “love” for palliative care that drew her back to Montreal and to her current position as medical director of St. Raphael’s.
As Lawlor provided me a tour of the care centre, which opened its doors in 2019 just before the COVID pandemic hit, it was abundantly evident the word is the best descriptor imaginable for her engagement with palliative care. She is candid that it can be, by its nature, an emotionally fraught relationship at times given that patients live on average 24 days (though some do get well enough to go home). One chronic frustration is not at the level of patient care but communicating to the broad public what palliative care actually comprises.
“One of the myths around palliative care is that it is what is done when ‘there is nothing left to be done,’ and this message is unfortunately reinforced in our medical language as people get sicker,” she says in a follow-up e-mail after my visit.
“For example, we still often hear medical professionals talk about ‘withdrawing care’ when in fact they are contemplating stopping certain invasive interventions. Or they refer to ‘level of care’ discussions when exploring what would more aptly be called the ‘level of intervention’ that is consistent with patient goals of care,” she adds.
St. Raphael’s is structured with great intentionality around leaving residents freedom to access what they deem necessary for their care by providing opportunities for art and music therapy and massage as well as physical spaces within the centre where they can gather with family members or friends to have precisely the kinds of conversations, or even just moments of togetherness, that Leonie Herx refers to.
“Care should not be equated with medical interventions,” Lawlor emphasizes. “Palliative care is not about withdrawing, abandoning, or ‘giving up.’ Unfortunately, this is still the message that many patients and their families receive.”
The extent to which MAiD has entered health care, she says, correlates with misidentifying palliative care as a form of “giving up,” with overmedication, and with the perceived or real abandonment of “patients and their families as they get sicker.”
Lawlor also casts a thought-provoking light on the limits of studies such as the one cited above from the CMAJ Open. While St. Raphael’s does have a partnership with both the McGill and Université de Montréal medical schools for regular experiential training of students and residents, it also “has trainees from the schools of nursing and social work at McGill, as well as trainees in massage therapy and music therapy, and eventually art therapy and acupuncture,” she notes.
“We plan on becoming a training site for various non-medical professions from business management to philanthropy, accounting, culinary training, and others.”
In other words, the widening net St. Raphael’s casts with its definition of care inside the centre extends outside as well, even to the prospect of partnerships with local elementary and high schools.
“The goal (would be) embedding the hospice within the community and demystifying palliative care while providing opportunities for learning, growth, and connection for everyone involved,” Lawlor says.
While that goal alone illuminates the future of palliative care with hope, what of the darker prospect of it becoming indistinguishable from MAiD, and the fate of B.C.’s Delta Hospice Society being replicated across the country. In Quebec, which along with B.C. has led the provinces in pushing the boundaries of medically administered death, there remains cautious optimism that palliative care can be protected.
Provincial law leaves private facilities free to refuse to MAiD requests, which so far acts as a buffer against subtle “suggestions” from Quebec City politicos and health care bureaucrats that it be it be made universal. Two members of St. Raphael’s board of directors are clear there are absolutely no plans to change the centre’s position that MAiD will remain outside its doors.
“We’ve discussed this over the years at the board, and we’re resolved that (palliative care) is what we do,” said Marco Ottoni, board vice-president and a founding member of St. Raphael’s. “You don’t go to a knee specialist to get shoulder surgery, right? So, people who come (to St. Raphael’s) understand we don’t offer MAiD. If they change their minds and want it, no problem, we follow the law and have a transfer set up to whatever hospital or institution’s going to do it. But irrespective of what individual opinions are, we don’t offer it.”
Ottoni said the board would naturally have to review its stance if Quebec law were changed, but right now it has far too much on its plate to get sidetracked by abstract possibilities. Likewise, board secretary Rita de Santis said the topic simply isn’t on the agenda now or in the foreseeable future.
De Santis, a lawyer and former member of Quebec’s National Assembly, said she voted in favour of MAiD when provincial law was changed to permit it six years ago. But she stressed that’s irrelevant to her board work for St. Raphael’s.
“It’s not on our agenda. We’re not discussing it, and I haven’t heard of any pressure from the government that would make us change that,” she said.
Out in British Columbia, Angelina Ireland says the Delta Hospice Society, too, will be steadfast in continuing bereavement and grief counselling as well as supportive therapies that were its core work before it fundraised $9 million to open the Irene Thomas palliative care centre a decade ago. The government has taken over the building and its contents, but that won’t prevent DHS from continuing to function.
“We will return to our roots helping people through the end-of-life journey,” Ireland says. “We won’t have (palliative care) beds because the government has made sure we won’t ever be able to do that again. They’ll put people to death by MAiD, and the people we used to care for will just be collateral damage. But our future is still in serving the community as best we can.”
Convivium publishes texts that do not necessarily reflect the views held by Cardus, the Convivium team, or its editors. In the spirit of discussion, dialogue, and debate, we ask readers to bear in mind that publication does not equal endorsement. Thanks for reading. Join the conversation!
Medically assisted death advocates inside and outside Parliament are gung-ho to expand it. But Cardus’ Ray Pennings says national poll numbers show Canadians want MPs to curb their enthusiasm.
Expansion of medically assisted dying risks an explosive moral crisis when shortages already endemic in health care make Canadians choose death over delay, Ruth Dick writes.
In Canada, access to palliative care varies from excellent to extremely poor based on where one lives yet euthanasia is now expected to be available anywhere at the first request
The Canadian Medical Association Journal (CMAJ) reported in 2010 that 32% of all assisted deaths (including euthanasia an...